As some of you know, I’ve recently become intrigued by the number of men I come across with some degree of Diastasis Recti. A DR is a split in the abdominal wall, which we commonly come across amongst pregnant and post-natal women.
DR is accepted/ expected as a normal result of pregnancy. As the baby grows, the abdominal wall splits to make room for the growing bump. Post-natal Pilates focuses on re-knitting the abdominal wall by gradually increasing loads to tone the abdominals whilst encouraging the abdominal wall to sink downwards and inwards. It’s a tricky balance. If you load too much, the abdominal wall is pushed outwards, further exacerbating the problem. If you load too little the client finds it very hard to ‘feel’ anything in the abdominals and other muscle groups like the Hip Flexors begin to take over.
The good thing is that when you work with a post-natal woman, they know that their abdominal wall is vulnerable. So they don’t go for broke on big abdominal exercises. They (often) listen to my instruction to reduce loading if they’re in a big class, or engage with the issue rather than trying to ignore it. Men with a DR, on the other hand, have not just given birth. They don’t feel vulnerable, in fact many of them appear to be quite strong. They often show up in my classes because their physio recommended Pilates for their lower back pain…small wonder. Many of them simply don’t accept that the abnormal bulge in their abdominal wall is a problem at all. The literature out there backs this up, calling it harmless. But a split in the fascial sheets of the abdominal wall is not functional. Try telling a buff looking man that he needs to do post-natal Pilates….
Enter Katy Bowman.
Katy Bowman is a bio-mechanist. She looks at movement in terms of forces placed on the bones, joints, soft-tissue and even the cells. Her philosophy is to develop nutritious movement habits, varying the loads and directions of pull on the body so that we develop a varied movement diet, leading to all-round wellbeing. She’s a massive fan of the squat and hanging from trees, for example, movements that our sedentary culture has made very easy to forgo.
In her most recent publication Diastasis Recti, Bowman insists that DR is a whole body problem. She identifies that all occurrences of DR result from too much pressure on the abdominal wall. Whether this is because of a growing baby in your belly, or if, like a friend of mine, you just picked up something too heavy and literally ‘bust your guts’. From a bio-mechanical point of view, the cause is the same: too much pressure on the abdominal wall from the inside outwards, and though the onset may be sudden, the fault lines have slowly been creeping up:
Slow sustained loads in a certain direction can deform tissues in a manner from which they cannot recover. Mechanical creep is the tendency of a material to deform slowly under a constant stress. The failure of a tissue in this case is called a creep failure. A diastasis recti or hernia is the result of creep failures.” Katy Bowman.
So Diastasis Recti is NOT just a natural result of pregnancy. It is the result of abnormal amounts of force on the abdominal wall, of which pregnancy may be one cause.
The abdominal muscles support the lower back. Poor tone or weakness in the abdominal wall results in a gradual wear and tear on the discs and intervertebral joints in the lower back. It’s obvious that a tear in the abdominal structures makes them a lot less functional (read: weak), which is why they really need to be addressed. I think that when medical professionals say that DR’s are ‘harmless’ what they mean is that they are not cancerous growths. But a DR is not something to ignore.
It follows that if the cause is the pressure on the abdominal wall, then just fixating on the location of the DR itself, as we tend to do with post-natal women, is a very limited way of looking at it. That doesn’t mean that specific, targeted abdominal work is not necessary. On the contrary, we do need to work to restore correct functioning of the abdominal muscles, but it needs to done within a program that considers the pressures on the abdominal wall brought about by the organization of the body as a whole.
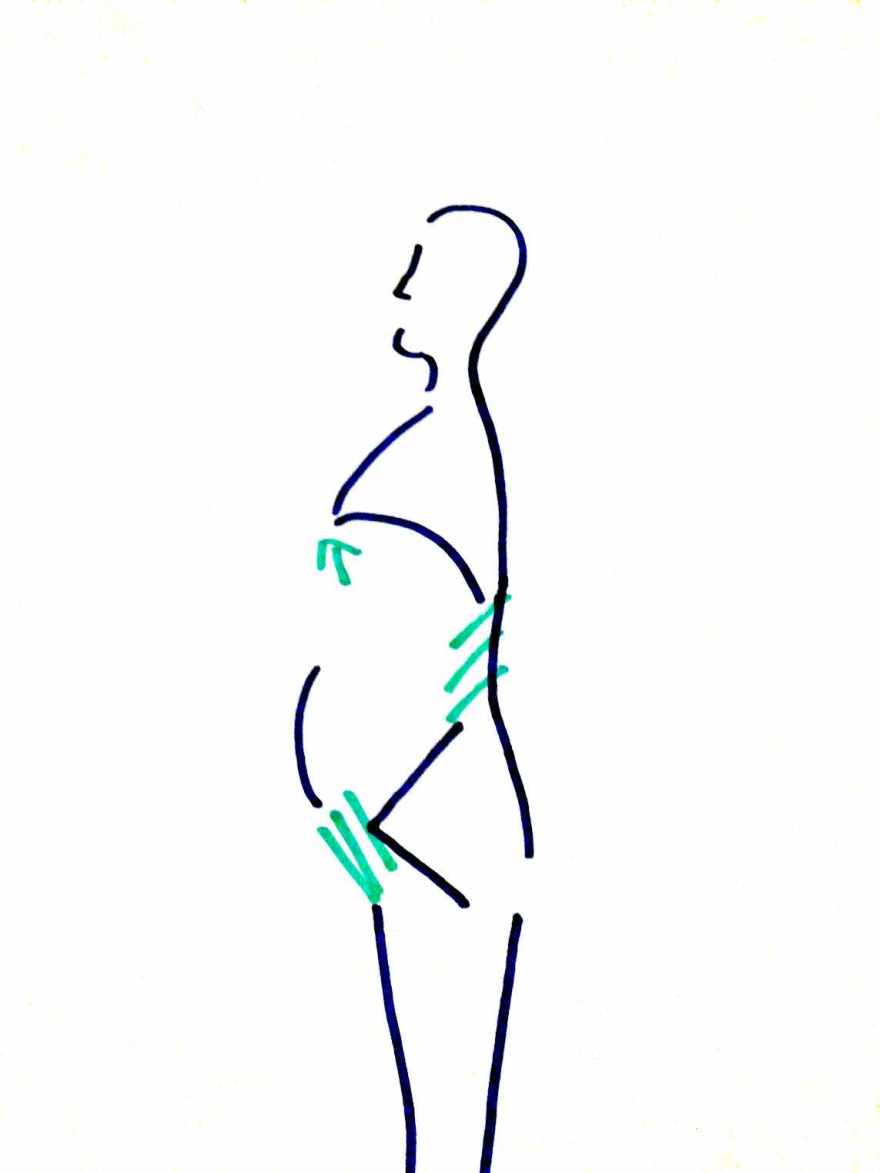
If I hold a picture  in my mind of clients who have a DR, the picture is roughly this. The rib cage is flailed, compressing the mid-back area and the pelvis is in a forward tilt. This appears to create more space out the front, making it the favoured posture for a pregnant woman. I think that men who adopt this posture (if they are not obese) do so because they may be trying to sit upright, but don’t have the mobility in their upper thoracic area or shoulders, and therefor hinge on the mid-back section. Once you displace the ribs in this way, it makes it very hard to feel a connection through the centre, so any abdominal work is likely to go into the Hip Flexors or lower back.
in my mind of clients who have a DR, the picture is roughly this. The rib cage is flailed, compressing the mid-back area and the pelvis is in a forward tilt. This appears to create more space out the front, making it the favoured posture for a pregnant woman. I think that men who adopt this posture (if they are not obese) do so because they may be trying to sit upright, but don’t have the mobility in their upper thoracic area or shoulders, and therefor hinge on the mid-back section. Once you displace the ribs in this way, it makes it very hard to feel a connection through the centre, so any abdominal work is likely to go into the Hip Flexors or lower back.
Bowman goes through a very comprehensive program of exercises to address every detail around this posture type, (and I highly recommend her book to clients, especially men, who have a DR). However, one of the key factors that makes DR quite difficult for a post-natal woman is: asymmetry, which I don’t think Bowman has addressed sufficiently in her book. Having one leg longer than the other, or some rotation in the pelvis, or a scoliosis all lead to a weakening of the abdominal wall. Lack of alignment causes weakness in the surrounding muscles. So addressing this is just as important. Once the body is aligned, the hip flexors are released and the ribs are dropped, we can then progress to more targeted abdominal work focusing on sinking the abdominal wall. The trajectory is therefor: align the pelvis, release the rib cage, open up the hip flexors and then integrate low level abdominal loads.
My next post will go into more detail on each of these. 🙂
